

All I know about cholesterol is that HDL should be high and LDL should be low. I don’t know what cholesterol actually does in your body. Is LDL low enough below some threshold, or is lower always better? Can LDL be too low? Also, what are triglycerides? And why isn’t the “total cholesterol” line on my blood work the sum of the HDL and LDL lines?
A marathon-running friend of mine who lives on kale, lentils, and olive oil has freakishly high HDL cholesterol. Could it be too high?
Let’s figure this out together. For my own reference, here are my most recent cholesterol results.
|
Dayton’s Cholesterol |
|
| LDL | 87 mg/dL |
| HDL | 62 mg/dL |
| Total | 157 mg/dL |
| Triglycerides | 42 mg/dL |
What is Cholesterol?
Cholesterol is in all of your cell membranes and “serves as a precursor for the biosynthesis of steroid hormones, bile acid and vitamin D” according to the Wikipedia article. Apparently cholesterol can be grouped into five kinds: chylomicrons, very-low-density lipoprotein (VLDL), intermediate-density lipoprotein (IDL), low-density lipoprotein (LDL), and high-density lipoprotein (HDL). The first two (I’ve never even heard of chylomicrons before) “deliver energy-rich triacylglycerol (TAG) to cells in the body” says UW. I guess TAG is another way of saying triglycerides. This Mayo Clinic page says your body uses triglycerides to store calories, especially from carbohydrates, that aren’t used immediately. Apparently your liver takes in these triglycerides and sends them back out as LDL cholesterol (LDL-C for short going forward), “to deliver cholesterol to cells, where it is used in membranes, or for the synthesis of steroid hormones.” Your liver also produces a chemical that binds to excess LDL-C to form HDL-C, which then returns to the liver and is removed from the bloodstream. So the crude model I have in mind now is that food becomes triglycerides, which become LDL-C, which becomes HDL-C, with your liver doing a lot of work along the way.
Calculation of Total Cholesterol
Total cholesterol is, of course, just the sum of the different kinds of cholesterol. It turns out that directly measuring every component of cholesterol is too expensive. What most labs do is measure total cholesterol, HDL and triglycerides. Then they estimate VLDL as one fifth of your triglycerides and calculate LDL as total cholesterol less VLDL and HDL It’s just an estimate, but it’s pretty accurate at much less cost.
Total Cholesterol
Early on, observational studies found that lower total cholesterol was correlated with lower mortality. This paper found that lower TC is better down to 180 mg/dL. This study of people in China with an average TC of about 150 mg/dL found that further decreases brought further benefits with “no evidence of any threshold.” Since then, there’s been more research broken down by type of cholesterol.
Triglycerides
Many web pages, recommend keeping triglycerides below 150 mg/dL. However, this gigantic meta-study of 61 prospective cohort studies through July 2013 found that people with triglycerides below 90 mg/dL were at 6% lower risk of all-cause mortality and 17% lower risk of mortality due to cardiovascular disease (CVD) compared to people in the range 90 – 150 mg/dL. People older or younger than 50 have the same effect size, but women are more sensitive to the harms of high triglycerides than men are.
This 2014 paper based on the Copenhagen City Heart Study uses a clever method called Mendelian randomization to test the causal relationship between triglycerides and all-cause mortality. Some people have alleles that cause them to have lower triglycerides without changing anything else about their bodies or causing them to behave differently (as far as we know). Nature has helpfully created a randomized controlled trial (RCT) for us. The study had a nice spread of people with between zero and six triglyceride-decreasing alleles. As expected, people with more of the alleles had progressively lower triglycerides. People with the most of these alleles lived three years longer than people with the fewest. This result, along with some more careful statistical analysis they did, strongly suggests the relationship between decreased triglycerides and decreased mortality is casual.
LDL Cholesterol
The best evidence on LDL cholesterol comes from RCTs of statins. This 2010 meta-analysis found that a low-dose statin reduces LDL by around 40 mg/dL and a high-dose statin reduces LDL by an additional 20 mg/dL. No matter what an individual’s baseline LDL was, every reduction by 40 mg/dL brought a 16% reduction in cardiac mortality, a 4% reduction in stroke mortality, and a 10% reduction in all-cause mortality. This result holds up very similarly for type-1 diabetics, type-2 diabetics, and non-diabetics; it holds up for people younger than 65 to older than 75; and for BMI below 25 to above 30. The benefit is slightly larger for men than women. Even for people with baseline LDL below 77 a 40 mg/dL reduction consistently provides >20% decrease in major cardiovascular events.
A pill that will lower nearly anyone’s total mortality risk by 10% is pretty amazing.
This follow-up analysis found that even the lowest-risk groups benefit from statins. They stratified patients by predicted 5-year major vascular event risk and found that the relative risk reduction was at least as large in the lowest risk groups as in the highest risk groups. They conclude that even for people with 5-year risk of a vascular event below 10%, “each 1·0 mmol/L [39 mg/dL] reduction in LDL cholesterol produces 11 fewer major vascular events per 1000 treated over 5 years, a benefit that greatly exceeds any known hazards of statin therapy.” Given that people in that low risk group typically do not receive statins, this is their way of saying way more people should take statins.
HDL Cholesterol
The effect of HDL cholesterol is not nearly as clear as LDL cholesterol. At the four year mark and again at the 12 year mark, the famous Framingham Heart Study found that higher HDL was correlated with lower risk of heart disease, whether or not you adjust for other health indicators like smoking, blood pressure, and weight. Around the same time, a similar study in Britain found that the benefit of HDL disappeared after adjusting for these other factors. This 1989 meta-study, which included both of these papers as well as two others, found that a 1 mg/dL increase in HDL was correlated with a 2-3% reduction in CVD mortality, even after adjusting for for other health indicators like blood pressure, smoking, and BMI.
This 2007 study specifically looked at about 2,700 people who took statins and successfully got their LDL below 70 mg/dL. If the benefit of HDL is that it “cleans out” LDL, then maybe there’s no benefit of having high HDL when you already have low LDL. That wasn’t what they found, though. The 80th percentile of HDL in this study was 55 mg/dL, just a bit lower than the recommended value of over 60. Among people with low LDL, those in the high HDL group were at 40% lower risk of CVD compared to people with HDL below 38 mg/dL. Still, none of this establishes causality. It also doesn’t tell us about the benefit or harm of getting HDL-C well above 60 mg/dL.
The experimental evidence for the effect of high HDL is more negative. This meta-study compiled 12 RCTs of drugs that raise HDL. These drugs did successfully raise HDL. However, across 54,000 patients, they found no evidence that raising HDL protects against total mortality or any of five secondary outcomes. This study doesn’t perfectly isolate increased HDL; it could be that these drugs have side effects that outweigh any benefits of HDL-C. Still, there were three different classes of drugs in these experiments and all three failed to provide any benefit on any measure whether considered separately or together. That’s a pretty resounding failure.
If raising HDL isn’t good for you, could it be that too much HDL is actually bad? This 2016 retrospective observational study with data on over 600,000 people found a U-shaped relationship between HDL and death from CVD, cancer, and all other causes. There are two problems with accepting this result at face value, as explained in that journal article and this popular one. 1) There’s no mechanism to explain why those sub-optimal HDL levels would be correlated with death from causes other than CVD and 2) low HDL is correlated with other behaviors that are known to be unhealthy. That hints that the correlation between HDL and mortality may not be causal. Exercise and moderate alcohol consumption, both of which are known to reduce CVD risk, raise HDL. Of course, it could be in part that they reduce your CVD risk precisely because they raise your HDL. Hard to tell without an RCT.
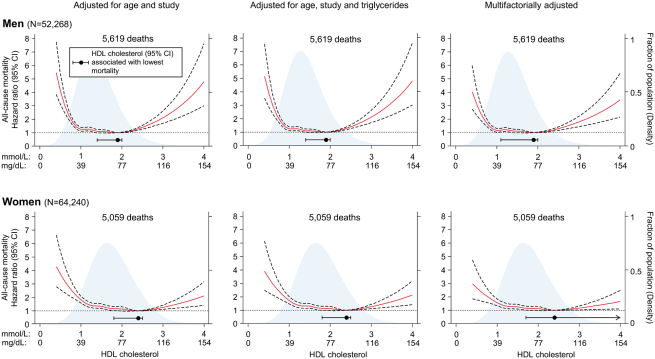
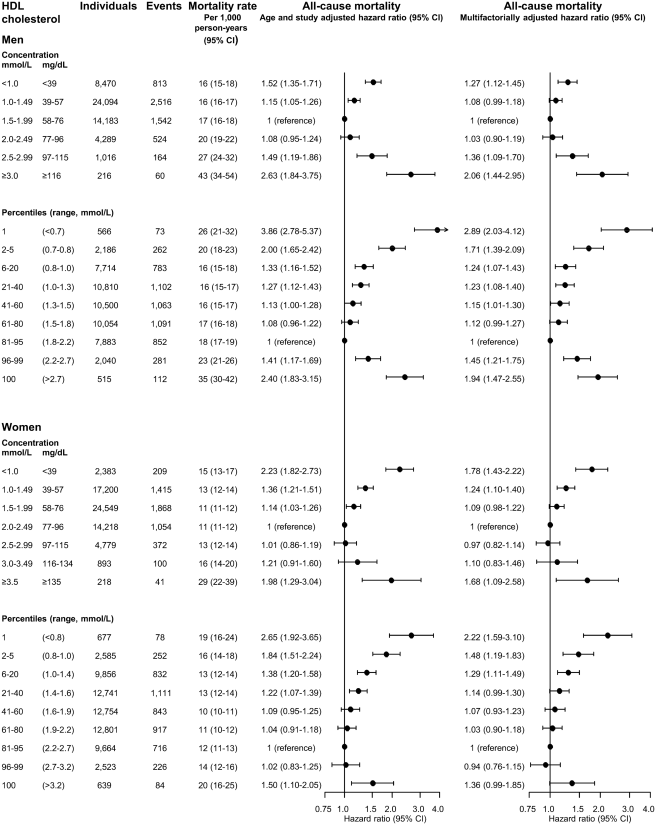
This 2017 meta-study of two prospective cohort studies in Denmark with a total of well over 100,000 people roughly confirmed the 2016 retrospective study. They found that the optimal HDL-C was 73 mg/dL for men and 93 mg/dL for women. They used some modeling to calculate mortality as a continuous function of HDL and simply broke people into groups by HDL-C. I’ll share their main figures below. (If you want to zoom in, you can find higher resolution versions here and here.) Finally, this 2018 prospective study in Britain found nearly identical results.
Bottom line, it seems like for men excessive HDL is definitely a concern and for women in might be a concern. In both cases, though, the relationship is unlikely to be causal. Don’t bother targeting a particular HDL level with drugs. Just follow the usual advice: don’t smoke, don’t eat trans fat, and get exercise. The Mayo Clinic says all those things contribute to higher HDL.
Final Recommendation
LDL: Should be as low as possible. The benefit is roughly linearly down to the lowest values anyone attains.
HDL: Ideally around 73 mg/dL for men and 93 mg/dL for women. It’s probably not causal, though, so don’t worry about it if you’re otherwise healthy.
Triglycerides: Ideally below 90 mg/dL.

{kind=link}
{kind=link}