

Powerful new drugs that reduce LDL cholesterol to unprecedented levels with minimal side effects should eliminate heart disease within the next few decades. The primary cause of heart disease is that excessive LDL cholesterol in the blood builds up as plaque inside blood vessels. In my last two posts, I wrote about the first- and second-line treatments to reduce LDL cholesterol: statins and ezetimibe. The LDL cholesterol in your blood mostly comes from your liver. Statins reduce your liver’s production of LDL. A smaller portion comes from cholesterol you eat. Ezetimibe works by preventing your body from absorbing dietary cholesterol. These drugs are fantastic. They’ve been studied in hundreds of thousands of people and found to reduce the risk of heart disease substantially with minimal side effects.
One of the key lessons from decades of studies is that when it comes to LDL cholesterol, lower is better. Experiments on these drugs started in people at high risk, often people with familial hypercholesterolemia, a genetic condition that drives LDL cholesterol extremely high. Over time, doctors have experimented with larger and larger doses and patients at lower and lower risk. They keep finding a benefit to lowering LDL cholesterol more and earlier in the progression of heart disease.
Residual risk
Statins and ezetimibe have not cured heart disease, though. The IMPROVE-IT trial was a large study of high-risk patients in which the treatment group received both a statin and ezetimibe. Over seven years, 13% had a heart attack and 4% had a stroke, lower than the control group but a lot higher than 0.
The treated patients ended with an average LDL cholesterol of 55 mg/dl. For comparison, vegans – who get no dietary cholesterol at all – average an LDL of 70 mg/dl, so LDL cholesterol of 55 mg/dl is likely unobtainable for the average patient without medication. If these drugs can already push LDL to unnaturally low levels, could there be a benefit to even further LDL reduction? Trials of a newer class of drugs, PCSK9 inhibitors, show us the answer is “yes”.
PCSK9 mutations
A bit like the movie Unbreakable, doctors figured that if some people have genes that push LDL cholesterol very high, there must be people who have genes that push it very low. How right they were. This Mendelian randomization study found that 3% of Black people in America have a “nonsense mutation” on one copy of the PCSK9 gene that makes it do nothing, with the result that their LDL cholesterol averages 100 mg/dl, versus 138 for similar people without the mutation. It also found that 3% of white people in America have a milder mutation on the PCSK9 gene that makes it do less, causing LDL to drop from an average of 137 to 116 mg/dl.
Of course, people have these genes their whole lives, so their cholesterol will be low from the time they’re born, not from the time a doctor prescribes them a statin. Over 15 years of follow-up, Black people with the nonsense mutation had an 89% reduction in heart disease risk. White people with the milder mutation had a 50% risk reduction.
Two teams of doctors – one in America and one in Zimbabwe – set out to find people with two copies of the nonsense mutation that drove cholesterol very low. Early in the 2000s, the two teams of doctors each discovered one healthy patient with LDL around 15 mg/dl who had inherited a rare gene from both their mother and father. The fact that they were perfectly healthy suggested there was no immediate danger to pushing LDL cholesterol so low. The story, recounted in this New York Times article, kicked off a search for drugs that would mimic the action of the genetic mutation.
Drugs to inhibit PCSK9
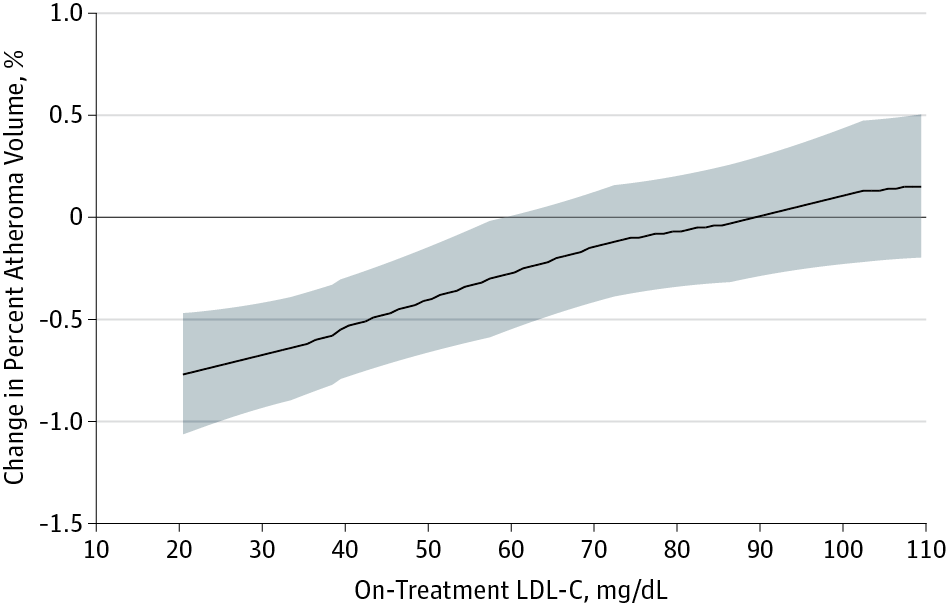
A randomized controlled trial (RCT) with around 1,000 patients studied one of the resulting drugs, monoclonal antibodies that inhibit PCSK9, to measure its effect on artery plaque buildup. The authors measured “percent atheroma volume,” the fraction of the vessel wall covered in atherosclerotic plaque. Their figure below shows how much the area of these plaques changed during the study as a function of the LDL level achieved. The breakeven point was about 90 mg/dl, with pretty wide uncertainty. Below, plaques regressed, above they grew. This result helps us think about which patients need to achieve what level of LDL. Patients who don’t already have significant plaque should stay that way as long as they keep LDL below about 90 mg/dl. But patients who already show signs of heart disease would likely benefit from getting LDL much lower to have their condition improve and not just stabilize.
Later, two large RCTs with a total of nearly 50,000 patients – the FOURIER trial and the ODYSSEY OUTCOMES trial – showed that PCSK9 inhibitors reduced LDL cholesterol by a huge 60% in patients who were already taking statins and had low baseline LDL cholesterol. Treated patients ended with a median LDL cholesterol of 30 mg/dl, a nearly impossible level to reach with prior drugs. The trials followed patients for about two and a half years and found a 20% reduction in a combined tally of outcomes like heart attack, stroke, and death from heart disease. They did not find a decrease in deaths from heart disease alone, though.
Why was the reduction in heart attack and stroke so much smaller than the reduction in LDL cholesterol? Why was there no reduction in death? One possible answer is that the follow-up period of two and a half years, compared to five years for the large statin trials, didn’t capture the full benefit. In the FOURIER trial, that 20% reduction in heart disease came from a 16% benefit in the first year and a 25% benefit after that. Amgen is running another trial with 13,000 lower-risk patients followed for four years to get a better measure of long-term outcomes. It’s scheduled to end in May 2025.
What’s the downside?
These drugs are given as injections once or twice a month, which may deter some patients. Both trials showed essentially no side effects besides about a 1% increase compared to placebo of patients reporting injection-site irritation. There were no increases in muscle problems, liver problems, or diabetes. The most significant side effect of statins – a small increase in type 2 diabetes – may develop over a longer timeframe than the length of these studies, so that can’t be ruled out yet.
The catch is cost. These drugs launched with a price of $14,600 per year. Predictably, insurance companies fought hard to prevent patients from getting them. Their reluctance is easy to understand. The results of the FOURIER study showed that 74 patients would need to be treated for two years – that’s $2.2 million at the initial list price – to avoid one major negative outcome. Also, these studies evaluated PCSK9 inhibitors as a supplement to statins, but ignored ezetimibe. Ezetimibe is a generic pill – essentially free compared to PCSK9 inhibitors – with roughly half the benefit.
In 2018, Amgen dropped the price of its drug to $5,850. In 2019, Sanofi matched that list price to the penny. This study covering data through mid-2019 found that only 2.5% of patients like those in the FOURIER and ODYSSEY trials were on the recommended PCSK9 therapy. This analysis finds that at the new price, PCSK9 inhibitors are cost-effective for very high risk patients. Hopefully access will improve in the future.
Near future of PCSK9 inhibition: from twice a month to twice a year
Existing PCSK9 inhibitors are monoclonal antibodies injected once or twice a month. The next PCSK9 inhibitor is inclisiran, a small interfering RNA drug (these words sound familiar from freshman biology but honestly I have no idea what they mean) that’s injected twice a year instead of twice a month. Inclisiran was approved in Europe in 2020. The FDA application was rejected not due to a problem with the drug but due to a problem with inspections at the manufacturing facility. The company says that should be fixed soon.
The ORION-10 and -11 trials, published in 2020, were two RCTs of inclisiran similar in setup to FOURIER and ODYSSEY. The trials took about 3,000 patients with high risk of heart disease but LDL cholesterol reasonably well managed by statins, then added inclisiran injections twice yearly. The result was a 50% reduction in LDL cholesterol, just a bit smaller than the 60% seen with the current drugs injected twice monthly. Just like the other drugs, the only side effect was about a 2% increase in injection site irritation. These studies only ran for 18 months and didn’t measure outcomes like heart attack and stroke, just focusing on LDL reduction.
This meta-analysis of three 18-month trials of inclisiran reports a 24% reduction in major adverse cardiovascular events, which would be a larger impact than the existing drugs. A much larger trial, ORION-4, will follow 15,000 patients for five years, scheduled to end in December 2024 (source) or maybe July 2026 (source). That study could pave the way for much more widespread adoption of inclisiran than any previous PCSK9 inhibitor.
Distant future of PCSK9 inhibition: from twice a year to once in a lifetime
The final destination on this journey of PCSK9 inhibition may be CRISPR base editing: a single injection that inhibits PCSK9 for a lifetime. These articles report on experiments in monkeys to knock out PCSK9. The company’s peer-reviewed paper reports LDL stayed 60% lower for at least eight months; the authors expect the change to be permanent. A press release from a few days ago claims those results were sustained through 15 months past injection and the company intends to start human trials in 2022.
A cure for heart disease?
The FOURIER and ODYSSEY trials showed that huge reductions in LDL cholesterol for patients who already have heart disease does not immediately cure them. But the Mendelian randomization study I shared above shows that keeping LDL cholesterol below a modest 100 mg/dl over a lifetime prevents nearly all heart disease. Combined with what we know about the development of plaques – they grow and shrink slowly – ending all heart disease will require keeping LDL cholesterol low for a lifetime, not just after patients show symptoms of heart disease.
The problem with sending LDL cholesterol near 0 in healthy young people is that it increases the risk of type 2 diabetes (T2D). Besides causing heart disease, T2D can also damage the eyes and kidneys, so we can’t ignore this side effect. If a single injection of a gene editor could send LDL cholesterol below 100 mg/dl for a lifetime, but not too much lower, that could eliminate nearly all cases of heart disease with only a small increase in T2D.
